

Stroke and TIA Survivors’ Perceptions of the COVID-19 Vaccine and Influences on Its Uptake: Cross Sectional Survey

Abstract
:1. Introduction
Stroke types
- -
- Ischaemic stroke: caused by a blockage cutting off the blood supply to the brain. This is the most common type of stroke.
- -
- Haemorrhagic stroke: caused by a bleeding in or around the brain.
- -
- Transient ischaemic attack (TIA): the same as a ischaemic stroke; however, symptoms last for a short amount of time because the blockage of blood supply to the brain is temporary.
Treatment for stroke
- -
- Thrombolysis: clot-busting drug which disperses the clot, usually given within 4.5 h
- -
- Thrombectomy: a treatment that physically removes a clot from the brain
- -
- Carotid endarterectomy: surgery to unblock fatty deposits from a carotid artery
- -
- Antiplatelet drug: help stop clots forming in the blood
- -
- Anticoagulant drug: help reduce their risk of developing new blood clots in the future
- -
- Blood pressure medicine: help lower high blood pressure
- -
- Cholesterol lowering drugs: help lower cholesterol
Stroke outcomes
- -
- Psychological impact: most common are anxiety and depression, but also anger, frustration, change in emotions
- -
- Cognitive impact: includes communication, spatial awareness, memory, concentration, executive function (ability to plan, solve problems and reason about situations) and praxis (ability to carry out skilled physical activities, such as getting dressed)
- -
- Physical problems: weakness, paralysis
- -
- Communication problems: problems with speaking, understanding reading and writing
- -
- Swallowing problems
- -
- Visual problems
- -
- Bladder and bowel control
2. Materials and Methods
2.1. Survey Development and Pre-Testing
2.2. Recruitment and Survey Administration
2.3. Context of Vaccine Roll Out
2.4. Patient and Public Involvement and Engagement
2.5. Data Analysis
3. Results
3.1. Quantitative Survey Questions
3.1.1. Vaccine Uptake
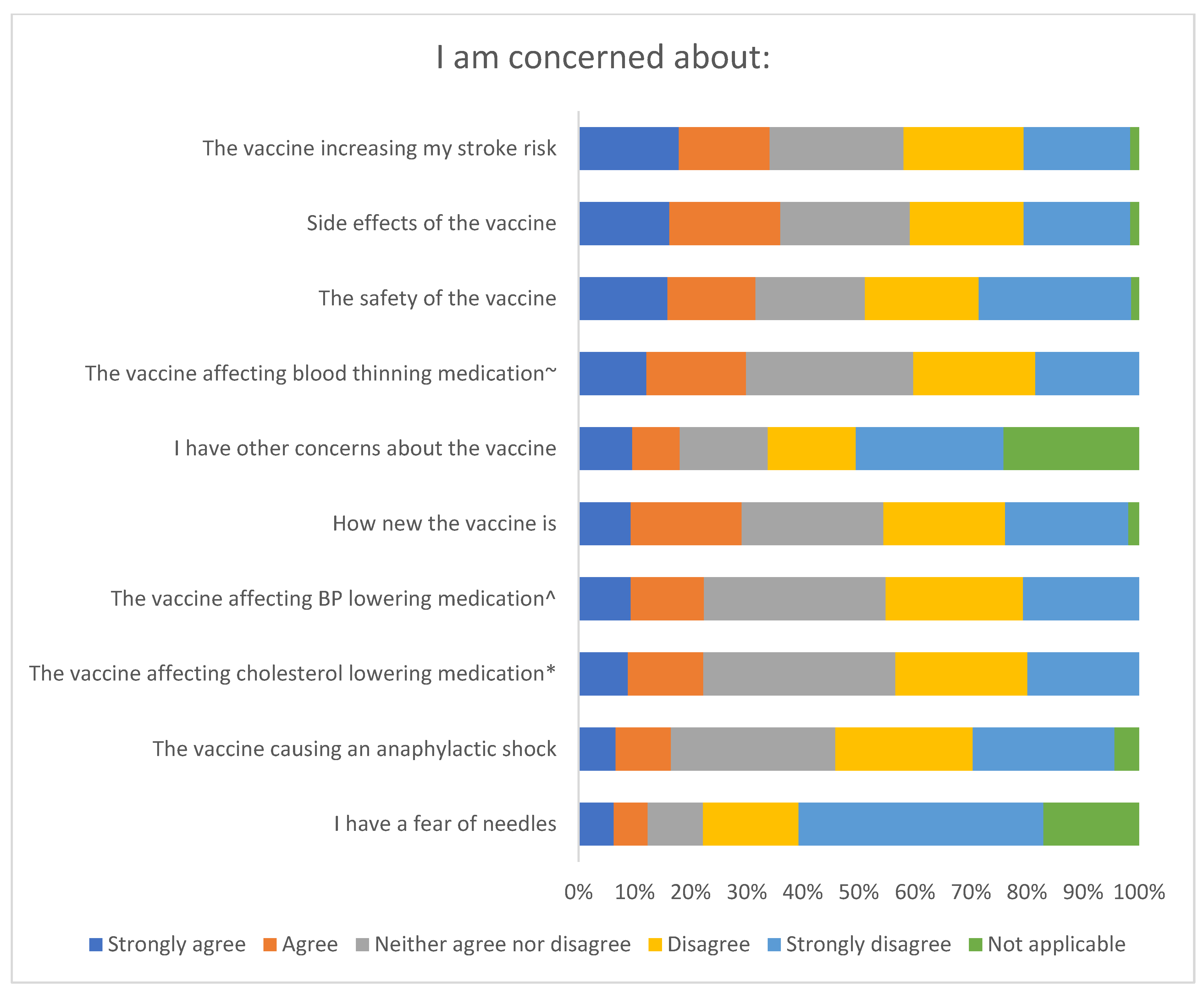
3.1.2. Perspectives of the Vaccine
Side Effects and Safety
- Side effects of the vaccine: 36.0% (131/364)
- The vaccine increasing their stroke risk: 34.1% (124/364)
- Safety of the vaccine: 31.6% (115/364)
- The vaccine affecting blood thinning medication: 29.9% (89/298)
- How new the vaccine is: 29.1% (106/364).
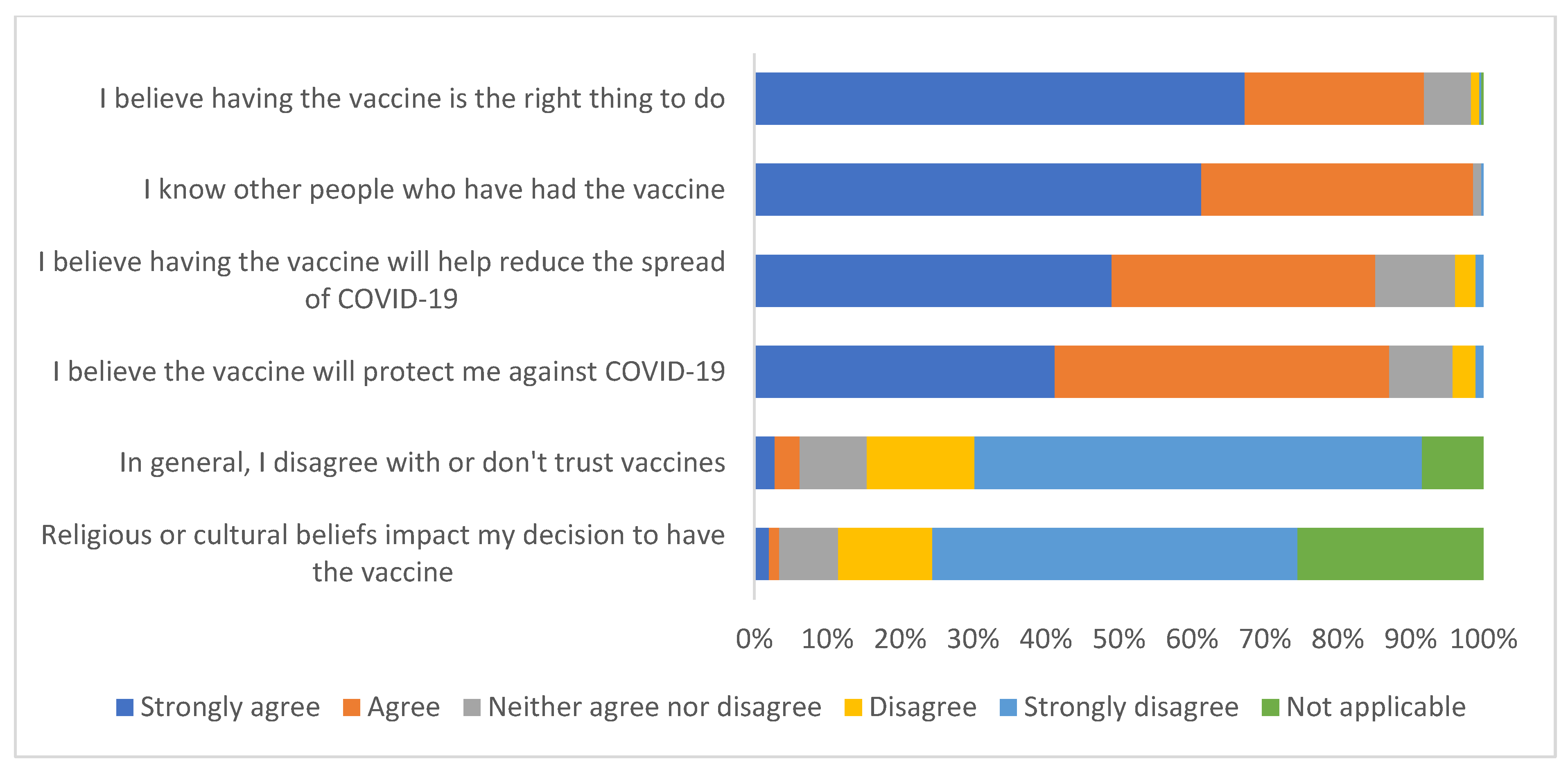
Beliefs and Social Influences
- Having the vaccine is the ‘right thing to do’: 91.8% (328/357)
- The vaccine will protect against COVID-19: 87.1% (311/357)
- The vaccine will help reduce spread of COVID-19: 85.1% (304/357).
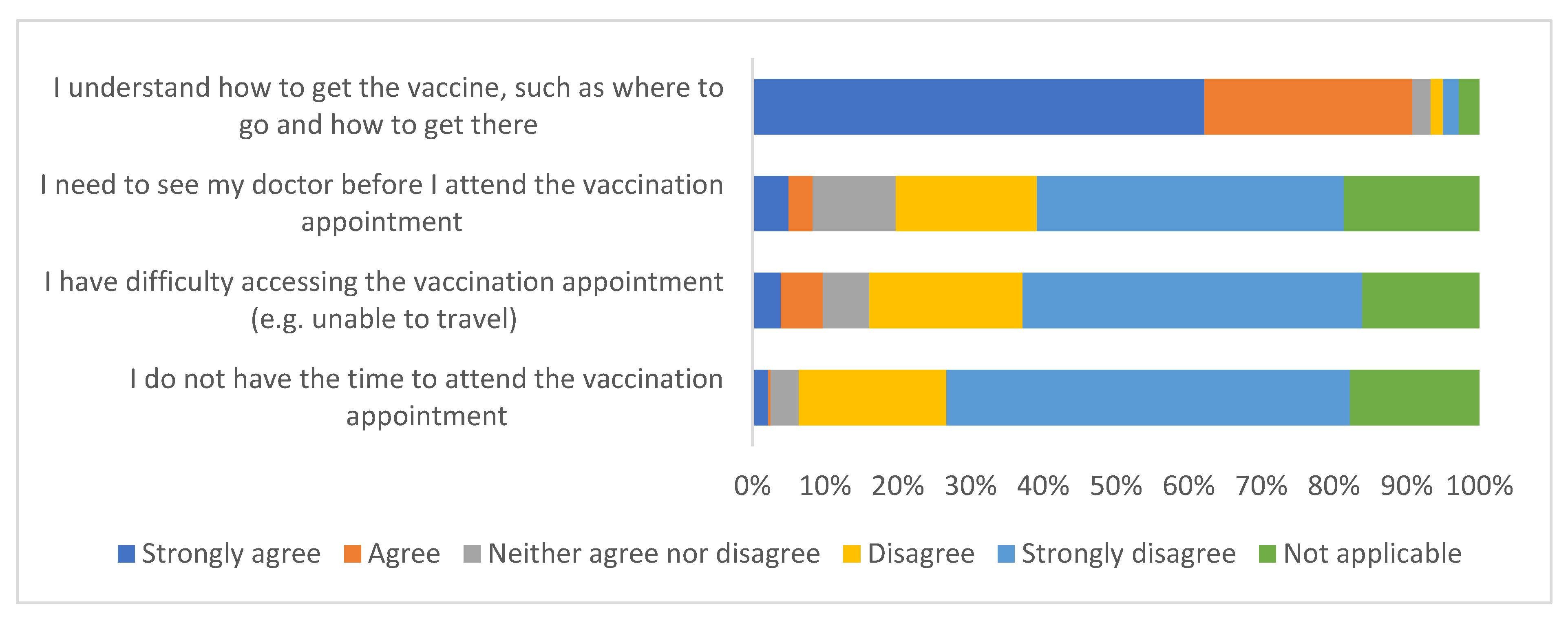
Access to the Vaccine Appointment
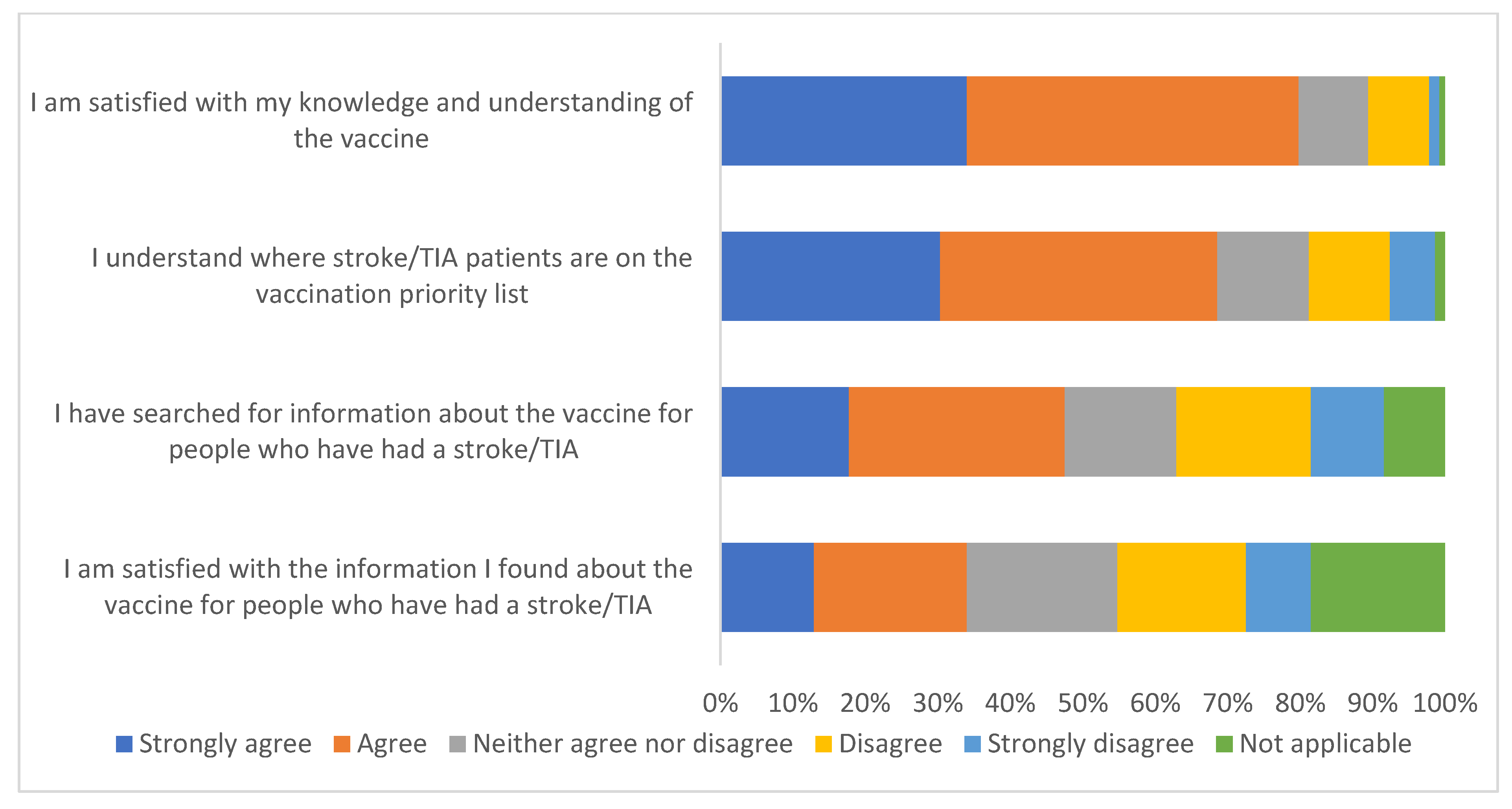
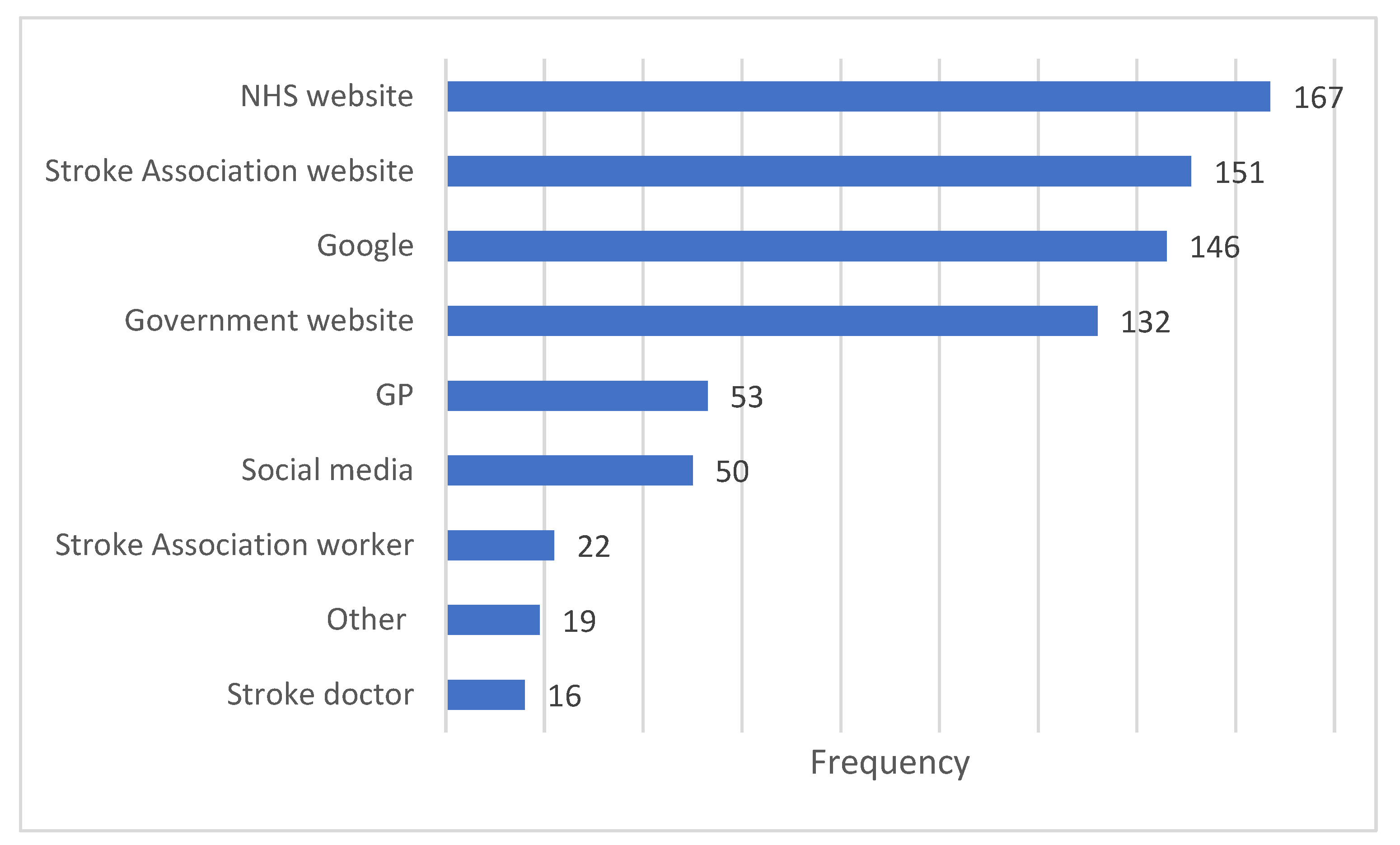
Knowledge and Understanding
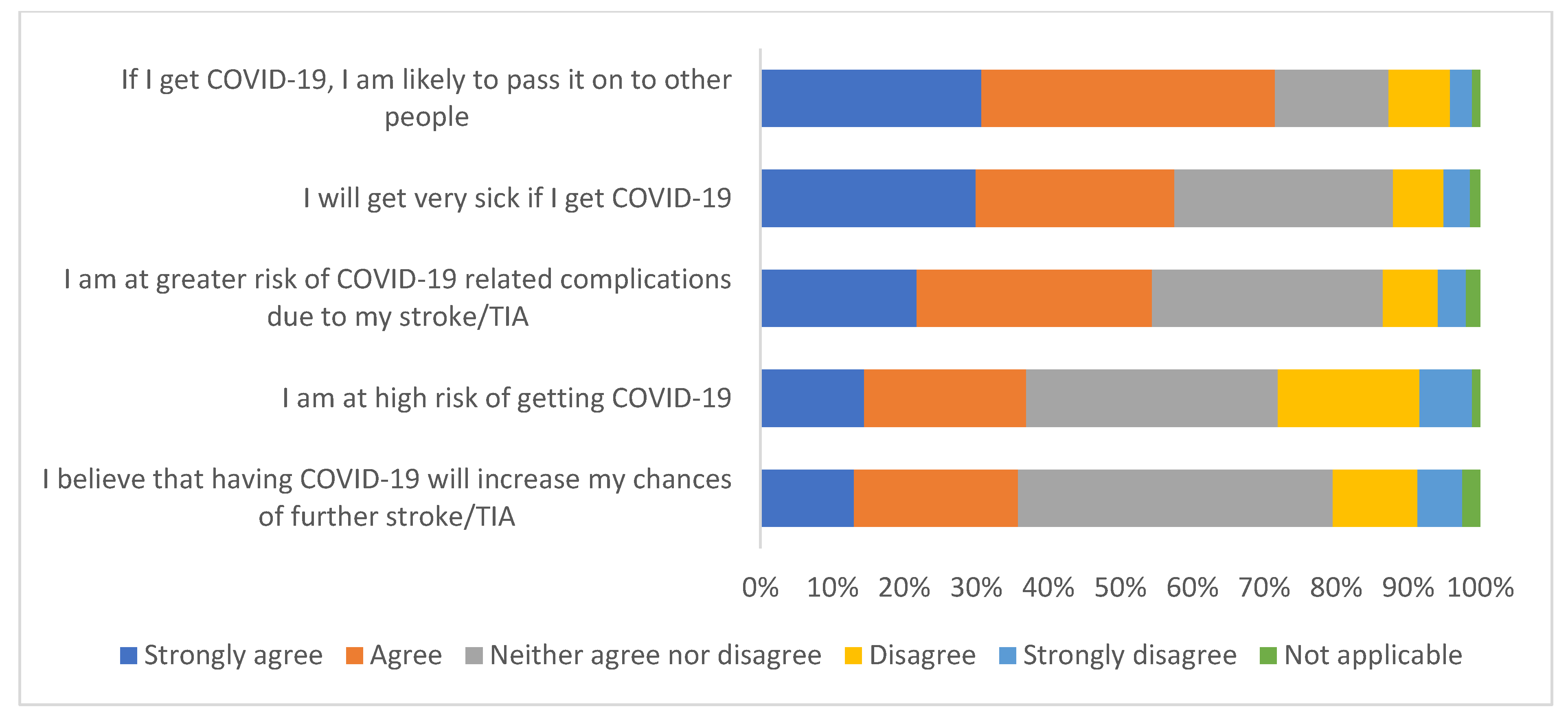
3.1.3. Perceptions of COVID-19
3.2. Qualitative Free Text Comments
3.2.1. Confidence
Blood Clots and Stroke Risk (COM-B: Motivation)
“Having had dose 1 of AstraZeneca vaccine prior to blood clot issues being reported I am very concerned as to the risks of my second vaccine. Very concerned when I previously had no hesitancy and am actually a vaccinator.”
“I had a mini stroke 1 week after receiving first dose. I refuse the second dose of Astrazenica [sic]. I am not being another death statistic.”
“17 days after having first vaccine AstraZeneca I had a TIA I am very worried about getting second jab. I’m almost certain it caused me to have a TIA.”
Side Effects and Safety (COM-B: Motivation)
“The vaccine first dose really put back my recovery by about 3 plus weeks increase in headaches and vertigo. I don’t know whether this means I should or shd [sic] not have second dose.”
“My other concerns were I was worried about my other health conditions and medication interfere with the vaccine.”
“Not sure that it is safe. Wondering if the whole world will be a grand science experiment as there is no long term study on any of the vaccines.”
Vaccine Side Effects
Mistrust of the Government/Vaccine and Non-Specified Concerns (COM-B: Motivation)
“I do not trust the goverment [sic] statistics. I don’t see any sign of a pandemic any more than the usual flu outbreaks we get yearly. I feel there is more to this than we are being told. I don’t like the fact we are being controlled and made to feel we have to have a vaccine in my body with pier [sic] pressure. Too many control measures being put on us.”
“I cancelled my first date because I was worried about having it [vaccine].”
Trust/Mistrust in the Vaccine’s Effectiveness (COM-B: Capability)
“The vaccine will reduce the impact of the virus thus preventing admission to hospital. The vaccine is not a cure.”
“It is not proven that by getting vaccinated or not is any less likely I wont [sic] get COVID [sic] or pass it on Testing is the best way not vaccination.”
3.2.2. Complacency
Value of the Vaccine: Social and Personal Motivations (COM-B: Opportunity/Motivation)
“The vaccine is the only way to get out of this pandemic.”
“If you want to see family members or friends you need to have the vaccine to protect them, although I was initially against having the vaccine.”
“I think people have the right to take the vaccine or not. I am concerned about the idea of stopping people getting jobs, going to restaurants, travelling etc if they do not have the vaccine.”
Perceived Personal Risk: Knowledge of COVID Risk Related to Stroke/TIA (COM-B: Capability/Motivation)
“I have no idea how COVID [sic] impacts on stroke survivors.”
“I had COVID [sic] in March 2020 and a tia [sic] in August. I believe COVID [sic] was the cause of my tia [sic]. I do not have a family history of strokes.”
“As i [sic] have other health issues aswell [sic] as stroke/TIA I was massively worried with how my body would cope with if i [sic] contracted COVID [sic].”
3.2.3. Convenience
Accessing the Appointment (COM-B: Capability/Opportunity)
“My carer arranged the appointment and the travel arrangements, all went smoothly.”
“Letter to request I book an appointment on line. I was offered [location A], [location B], [location C], [location D] and some others all miles from my home town. I rang telephone advice line to be told I would have to wait for my doctor or local NHS to contact me for a local appointment. No-one seemed concerned that I was shielding and very vulnerable. It was two weeks later that by telephone I was offered a local appointment.”
“I was surprised to only just learn that as a stroke survivor, I am in group 6 for the vaccine rollout. Disappointed to have not been invited for the vaccine by my GP.”
Accessing Information (COM-B: Capability/Opportunity)
“I didn’t research having the vaccine. I believed that what ever [sic] the effects would be I would ultimately be in a better position for having it than I would of been not having it.”
“I have accessed general information on line but feel my GP surgery should inform its stroke patients with more personalised advice and information for individuals.”
“I contacted my doctor to discuss my jab, but couldn’t get an appointment because the surgery wasn’t really interested in my concerns! No discussion, just a receptionist who said it was safe to have the vaccine! No reassurance for me at all.”
“I have researched about COVID [sic] and l know that can give blood clots. There is such a lack of advice out there.”
“I struggle with information since my strokes hard to take it in an understand it.”
Knowledge about Where Stroke Was on Priority List (COM-B: Capability)
“As far as I am aware people who have had a stroke or TIA were not on a priority list.”
4. Discussion
4.1. Principal Findings
4.2. Strengths and Weaknesses
4.3. Comparison with Other Studies
4.4. Implications for Clinicians and Policymakers
4.5. Unanswered Questions and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Williams, R.; Jenkins, D.A.; Ashcroft, D.M.; Brown, B.; Campbell, S.; Carr, M.J.; Cheraghi-Sohi, S.; Kapur, N.; Thomas, O.; Webb, R.T.; et al. Diagnosis of physical and mental health conditions in primary care during the COVID-19 pandemic: A retrospective cohort study. Lancet Public Health 2020, 5, e543–e550. [Google Scholar] [CrossRef]
- Abrams, E.M.; Szefler, S.J. COVID-19 and the impact of social determinants of health. Lancet Respir. Med. 2020, 8, 659–661. [Google Scholar] [CrossRef]
- Shih, H.-I.; Wu, C.-J.; Tu, Y.-F.; Chi, C.-Y. Fighting COVID-19: A quick review of diagnoses, therapies, and vaccines. Biomed. J. 2020, 43, 341–354. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- World Health Organisation. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 27 September 2022).
- World Health Organisation. Who Are at Higher Risk of Developing Serious Illness from COVID-19. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 27 September 2022).
- Rzymski, P.; Zeyland, J.; Poniedziałek, B.; Małecka, I.; Wysocki, J. The Perception and Attitudes toward COVID-19 Vaccines: A Cross-Sectional Study in Poland. Vaccines 2021, 9, 382. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12, 21501327211013303. [Google Scholar] [CrossRef] [PubMed]
- Gadoth, M.A.; Halbrook, M.M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, M.A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- NHS. People at Higher Risk from Coronavirus (COVID-19). Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/people-at-higher-risk/ (accessed on 27 September 2022).
- Bhugra, P.; Grandhi, G.R.; Mszar, R.; Satish, P.; Singh, R.; Blaha, M.; Blankstein, R.; Virani, S.S.; Cainzos-Achirica, M.; Nasir, K. Determinants of Influenza Vaccine Uptake in Patients With Cardiovascular Disease and Strategies for Improvement. J. Am. Heart Assoc. 2021, 10, e019671. [Google Scholar] [CrossRef]
- Aggarwal, G.; Lippi, G.; Henry, B.M. Cerebrovascular disease is associated with an increased disease severity in patients with Coronavirus Disease 2019 (COVID-19): A pooled analysis of published literature. Int. J. Stroke 2020, 15, 385–389. [Google Scholar] [CrossRef]
- Nalleballe, K.; Siddamreddy, S.; Sheng, S.; Dandu, V.; Arulprakash, N.; Kovvuru, S.; Kamran, M.; Jasti, M.; Onteddu, S. Coronavirus Disease 2019 in Patients With Prior Ischemic Stroke. Cureus 2020, 12, e10231. [Google Scholar] [CrossRef]
- British Association of Stroke Physicians. COVID-19. Available online: https://www.basp.org/covid-19/ (accessed on 27 September 2022).
- Stroke Association. Stroke and the Coronavirus 2021. Available online: https://www.stroke.org.uk/finding-support/stroke-and-coronavirus-vaccine (accessed on 27 September 2022).
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Stroke Association. Available online: https://www.stroke.org.uk/ (accessed on 27 September 2022).
- NHS. Stroke. Available online: https://www.nhs.uk/conditions/stroke/ (accessed on 27 September 2022).
- Public Health England. COVID-19 Vaccination First Phase Priority Groups 2021. Available online: https://www.gov.uk/government/publications/covid-19-vaccination-care-home-and-healthcare-settings-posters/covid-19-vaccination-first-phase-priority-groups (accessed on 27 September 2022).
- BBC. COVID: 30 Blood Clot Cases Found in Astrazeneca Recipients in the UK: BBC. 2021. Available online: https://www.bbc.co.uk/news/health-56616119 (accessed on 27 September 2022).
- Daily Mail. Urgent Probe is Launched into ‘Link’ between Astrazeneca Vaccine and Man Who Was Rushed to Hospital after Receiving the Jab—As Top Doctor Reveals the Warning Signs to Watch Out 2021. Available online: https://www.dailymail.co.uk/news/article-9431583/Urgent-probe-launched-AstraZeneca-Covid-vaccine-man-rushed-hospital-blood-clots.html (accessed on 27 September 2022).
- Kyngäs, H.; Kaakinen, P. Deductive Content Analysis. In The Application of Content Analysis in Nursing Science Research; Kyngäs, H., Mikkonen, K., Kääriäinen, M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 23–30. [Google Scholar]
- Razai, M.S.; Osama, T.; McKechnie, D.G.J.; Majeed, A. Covid-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- ONS. Coronavirus and Vaccine Hesitancy, Great Britain: 31 March to 25 April 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandvaccinehesitancygreatbritain/31marchto25april (accessed on 27 September 2022).
- NHS. COVID-19 Vaccination Statistics 2021. Available online: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2021/04/COVID-19-weekly-announced-vaccinations-29-April-2021.pdf (accessed on 27 September 2022).
- Moore, R.; Purvis, R.S.; Hallgren, E.; Willis, D.E.; Hall, S.; Reece, S.; CarlLee, S.; Judkins, H.; McElfish, P.A. Motivations to Vaccinate Among Hesitant Adopters of the COVID-19 Vaccine. J. Community Health 2021, 47, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; Duffy, B.; Moxham-Hall, V.; McAndrew, S.; Murkin, G. COVID-19 Vaccines: Confidence, Concerns and Behaviours. 2021. Available online: https://www.kcl.ac.uk/policy-institute/assets/covid-19-vaccines-confidence-concerns-behaviours.pdf (accessed on 27 September 2022).
- Marcec, R.; Likic, R. Using Twitter for sentiment analysis towards AstraZeneca/Oxford, Pfizer/BioNTech and Moderna COVID-19 vaccines. Postgrad. Med. J. 2021, 98, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.H.; Pickles, K.; Nickel, B.; Cvejic, E.; Ayre, J.; Batcup, C.; Bonner, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Concerns and motivations about COVID-19 vaccination. Lancet Infect. Dis. 2021, 21, 161–163. [Google Scholar] [CrossRef]
- Eibensteiner, F.; Ritschl, V.; Nawaz, F.A.; Fazel, S.S.; Tsagkaris, C.; Kulnik, S.T.; Crutzen, R.; Klager, E.; Völkl-Kernstock, S.; Schaden, E.; et al. People’s Willingness to Vaccinate Against COVID-19 Despite Their Safety Concerns: Twitter Poll Analysis. J. Med. Internet Res. 2021, 23, e28973. [Google Scholar] [CrossRef]
- Chun, H.Y.; Whiteley, W.N.; Dennis, M.S.; Mead, G.E.; Carson, A.J. Anxiety After Stroke: The Importance of Subtyping. Stroke 2018, 49, 556–564. [Google Scholar] [CrossRef]
- Germani, F.; Biller-Andorno, N. The anti-vaccination infodemic on social media: A behavioral analysis. PLoS ONE 2021, 16, e0247642. [Google Scholar] [CrossRef]
- Prieto Curiel, R.; González Ramírez, H. Vaccination strategies against COVID-19 and the diffusion of anti-vaccination views. Sci. Rep. 2021, 11, 6626. [Google Scholar] [CrossRef]
- Pullan, S.; Dey, M. Vaccine hesitancy and anti-vaccination in the time of COVID-19: A Google Trends analysis. Vaccine 2021, 39, 1877–1881. [Google Scholar] [CrossRef]
- Hamel, L.; Lopes, L.; Sparks, G.; Kirzinger, A.; Kearney, A.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: January 2022. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-january-2022/ (accessed on 27 September 2022).
- Davis, C.J.; Golding, M.; McKay, R. Efficacy information influences intention to take COVID-19 vaccine. Br. J. Health Psychol. 2021, 27, 300–319. [Google Scholar] [CrossRef] [PubMed]
- Stadnick, N.A.; Cain, K.L.; Oswald, W.; Watson, P.; Ibarra, M.; Lagoc, R.; Ayers, L.O.; Salgin, L.; Broyles, S.L.; Laurent, L.C.; et al. Co-creating a Theory of Change to advance COVID -19 testing and vaccine uptake in underserved communities. Health Serv. Res. 2022, 57 (Suppl. 1), 149–157. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Lam, K.; Danielli, S.; Ashrafian, H.; Darzi, A. COVID-19 vaccinations among Black Asian and Minority Ethnic (BAME) groups: Learning the lessons from influenza. Int. J. Clin. Pract. 2021, 75, e14641. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | ||
|---|---|---|
| Diagnosis | Stroke | 253 (67.1) |
| TIA | 67 (17.8) | |
| Both | 47 (12.5) | |
| Unsure | 10 (2.7) | |
| Gender | Male | 163 (43.2) |
| Female | 213 (56.5) | |
| Non-binary | 1 (0.3) | |
| Age | 18–25 years | 3 (0.8) |
| 26–35 years | 7 (1.9) | |
| 36–45 years | 30 (8.0) | |
| 46–55 years | 95 (25.2) | |
| 56–65 years | 130 (34.5) | |
| 66–75 years | 73 (19.4) | |
| 76–85 years | 38 (10.1) | |
| ≥86 years | 1 (0.3) | |
| Ethnicity | White | 362 (96.0) |
| Mixed/multiple ethic groups | 3 (0.8) | |
| Asian/Asian British | 5 (1.3) | |
| Black/African/Caribbean/Black British | 5 (1.3) | |
| Prefer not to say | 2 (0.5) | |
| Highest level of education | No formal qualification | 36 (9.6) |
| GCSE/O-Levels/CSE/Foundation Diploma | 100 (26.5) | |
| Apprenticeship | 15 (4.0) | |
| AS/A-Levels/BTEC/Advanced NVQs | 72 (19.1) | |
| Degree (e.g., BA/BSc) | 92 (24.4) | |
| Higher Degree (e.g., MSc/PhD) | 36 (9.6) | |
| Other | 26 (6.9) | |
| Employment status | Employed-full time | 80 (21.2) |
| Employed-part time | 37 (9.8) | |
| Furloughed-full time | 6 (1.6) | |
| Furloughed-part time | 6 (1.6) | |
| Volunteer | 13 (3.4) | |
| Housewife/househusband | 5 (1.3) | |
| Unemployed | 46 (12.2) | |
| Retired | 162 (43.0) | |
| Student | 4 (1.1) | |
| Other | 18 (4.8) | |
| Experienced COVID-19 | Yes | 44 (11.7) |
| No | 297 (78.8) | |
| Unsure | 36 (9.6) |
| n (%) | |
|---|---|
| Yes-first dose | 307 (81.4) |
| Yes-first and second dose | 12 (3.2) |
| No-I’ve not been offered it yet | 30 (8.0) |
| No-But booked to have vaccine | 9 (2.4) |
| No-I declined the vaccine | 7 (1.9) |
| No-I’ve been offer it but not taken up yet | 11 (2.9) |
| No-Other | 1 (0.3) |
| 3C’s Vaccine Hesitancy Model | COM-B | Intervention Functions | Example |
|---|---|---|---|
| Confidence-vaccine safety | Capability-know the vaccine is safe Motivation-do not have overwhelming fear of the vaccine | Education | Provide clear, concise information on the vaccine and risk of stroke/blood clots, preferably specific to stroke/TIA survivors. Information should be up-to-date and regularly updated as new research emerges. Information should use lay language, be co-produced with patients and be presented visually (e.g., infographics) and using illustrative analogies to contextualise information. Information should be easily available, such as on trusted NHS government websites. Information should be adapted to accommodate accessibility considerations (e.g., visual problems) and stroke-related impairments (e.g., cognitive problems). Empower families/carers to support people with stroke with their information needs. |
| Education | Initial information provision in the acute setting is crucial and individual concerns/questions can be discussed. Proactively target newly diagnosed stroke/TIA patients to dispel misinformation about their stroke being related to the vaccine and to promote uptake of the second vaccine. A summary of this information should be included in the discharge letter. | ||
| Education | Educate healthcare providers and vaccinators to provide information to address vaccine safety concerns, particularly regarding blood clot and stroke risk—i.e., more than the top line message ‘the vaccine is safe’. Concerns should be acknowledged and not dismissed. As trusted information sources, healthcare providers should have knowledge of where to access up-to-date, evidence-based information. | ||
| Environmental restructuring | Improve access to personalised advice, support and reassurance from trusted individuals, such as GPs or the Stroke Association helpline. | ||
| Complacency-perceived risk of COVID | Capability-understand personal risks Motivation-perceive COVID as health risk | Education | Increase knowledge of the greater risks of complications from contracting COVID-19 for individuals who have had a stroke/TIA. Focus messaging on ‘get the vaccine to reduce your risk’. |
| Complacency-perceived value of the vaccine | Motivation | Persuasion | Communicate social responsibility and personal benefit to induce positive feelings and stimulate vaccination uptake. |
| Modelling | Publicise positive stories of vaccine uptake in stroke/TIA survivors as examples for people to aspire to. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turner, G.M.; Heron, N.; Crow, J.; Kontou, E.; Hughes, S. Stroke and TIA Survivors’ Perceptions of the COVID-19 Vaccine and Influences on Its Uptake: Cross Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 13861. https://doi.org/10.3390/ijerph192113861
Turner GM, Heron N, Crow J, Kontou E, Hughes S. Stroke and TIA Survivors’ Perceptions of the COVID-19 Vaccine and Influences on Its Uptake: Cross Sectional Survey. International Journal of Environmental Research and Public Health. 2022; 19(21):13861. https://doi.org/10.3390/ijerph192113861
Chicago/Turabian StyleTurner, Grace M., Neil Heron, Jennifer Crow, Eirini Kontou, and Sally Hughes. 2022. "Stroke and TIA Survivors’ Perceptions of the COVID-19 Vaccine and Influences on Its Uptake: Cross Sectional Survey" International Journal of Environmental Research and Public Health 19, no. 21: 13861. https://doi.org/10.3390/ijerph192113861